

The idea behind a single-payer health care system is simple: Have one entity pay for all health care. The result would be universal health insurance or coverage for all. This idea has long been politically unfeasible because it was considered to cost too much, disrupt almost 20 percent of the economy, and eliminate the need for employer-sponsored health insurance, which covers about half of all Americans.
However, dissatisfaction with the current multi-payer health insurance system and the recent failure of Congress to repeal and replace the Affordable Care Act has emboldened more Democrats in Congress to support the approach. Sen. Bernie Sanders (I-Vermont) on Wednesday unveiled a bill (CBS) that takes a “Medicare for All” approach to single-payer. (Check out his op-ed in Wednesday’s New York Times and his Facebook page announcement.)
The bill largely builds on Medicare’s existing infrastructure, which today primarily covers senior citizens. As the Washington Post’s David Weigel notes in a preview of the legislation, “Sanders’s bill, the Medicare for All Act of 2017, has no chance of passage in a Republican-run Congress” but sets up the issue for Democrats to run on in 2018 mid-term elections and the 2020 presidential campaign.
Just last week, Max Baucus, the fiscally moderate former Democratic senator from red-state Montana, expressed his support for single-payer, according to reporting by Gail Schontzler of the Bozeman Daily Chronicle. “It was a startling turnaround for Baucus, who eight years ago was chairman of the powerful Senate Finance Committee and a key Democratic leader in the political battles that ultimately passed the Affordable Care Act,” she wrote.
If Baucus had stayed in the Senate, he’d might have joined a growing number of colleagues in the progressive wing of his party signing on to single-payer, including Sens. Corey Booker (New Jersey), Kamala Harris (California), Chris Murphy (Connecticut) and Elizabeth Warren (D-Mass.).
In the U.S. House of Representative, Rep. John Conyers (D-Michigan) is sponsoring a similar Medicare-centric single-payer bill, the H.R. 676, Expanded & Improved Medicare for All Act, which has more than 100 cosponsors.
Shifting the health care system, which in 2015 reached $3.2 trillion or 17.8 percent of the U.S. economy, away from the combination of private commercial insurers and public payers to single payer is no small task, as Jeff Stein explained in an article for Vox last month. He outlined five significant policy hurdles, saying any such system would need:
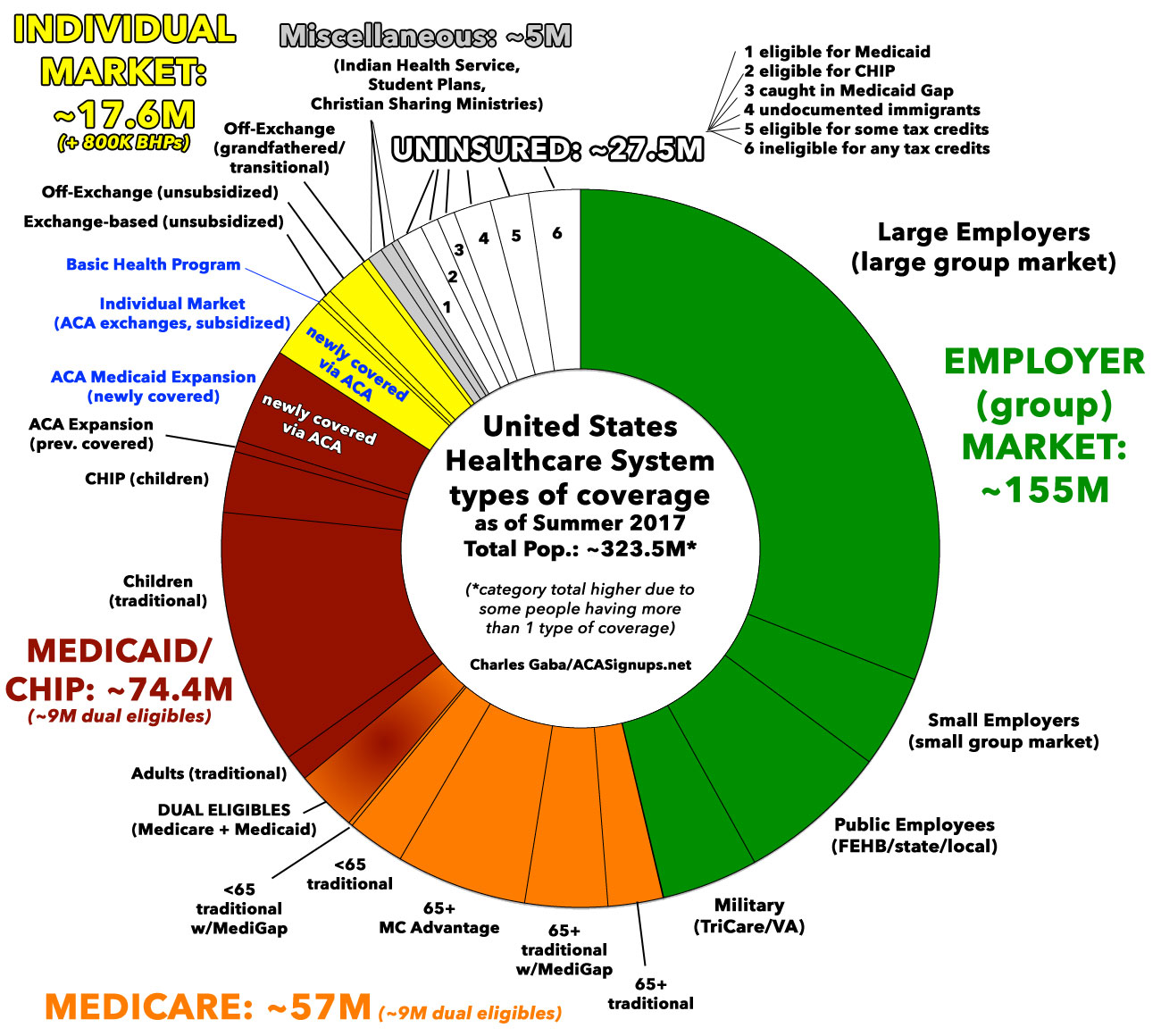
- To establish a new government insurer for all 330 million Americans when employers cover about 153 million Americans (47 percent), the government-funded Medicaid and Medicare cover 38 percent, private insurers enroll 5 percent on the ACA’s Marketplace exchanges and 9 percent remain uninsured.
- Put hundreds of millions of people onto a new government program overnight.
- Pay for government insurance for everyone.
- Establish a new federal infrastructure to manage everyone’s insurance
- Make for-profit providers illegal, then retrain and re-employ those who lose their jobs as a result.

On Monday, the NYT’s David Leonhardt took a similar approach in his article, 5 Questions About Single-Payer Health Care. One of the toughest of the five questions was this: Can single-payer overcome its political obstacles? “The recent failure of statewide single-payer proposal in Sander’s left-leaning Vermont, which helped end the governor’s political career, shows how brutal the politics are,” he wrote.
For The Atlantic, Olga Kazan addressed the issue of how to shift from the current multi-payer mechanism to single-payer. Would Congress vote for and Trump sign a bill calling for Medicare for all if Medicare pays less than most health plans and employers pay for physician and hospital care, she asked. Health insurance consultant Robert Laszewski told her, “Now, call a hospital administrator and tell him that his reimbursement for all the employer-based insurance he gets now is going to be cut by 50 percent, and ask him what’s going to happen,” he said. “I think you can imagine—he’d go broke.”
But before any hospital or physician goes broke, lobbyists for hospitals, insurers and physician groups would likely oppose such a bill.
Consider what happened in the early 1990s when then-President Clinton proposed a health care reform. Insurance companies funded ads that hammering home the message that the Clinton plan was something to be feared. (Here’s a compilation of ads that ran at the time.)
To be sure, not all physicians oppose single-payer. Physicians for a National Health Program have long favored single-payer as the group explains here. Also, more than half of physicians responding to a recent survey said they favored single-payer. In an article for California Healthline, Rachel Bluth wrote, “Fifty-six percent of doctors registered either strong support or were somewhat supportive of a single-payer health system, according to the survey by Merritt Hawkins, a physician recruitment firm. In its 2008 survey, opinions ran the opposite way: 58 percent opposed single-payer.” Here’s a report on the Merritt Hawkins survey.
However, physicians are just one constituent group. Any single-payer plan also will need more political support, as President Obama found when he worked with the Democrats in Congress to pass the ACA in 2010. At Vox, Sarah Kliff recounted that history in a Monday tweet.
Another politician who recognizes the inherent danger in supporting single payer is first-term Sen. Chris Murphy (D-Conn.). Espousing a pragmatic approach, as Elana Schor reported for Politico, Murphy is preparing to introduce legislation this fall to let individuals and businesses buy into Medicare through the ACA’s Marketplace exchanges, she wrote. This approach is, “designed to get Democrats closer to that lofty but potentially unobtainable goal” of single payer.
Indeed, the politics are challenging, as single-payer expert William Hsiao, Ph.D., outlined during a presentation last month in Brewster, Mass. Hsiao, the K.T. Li Research professor of economics at the Harvard T.H. Chan School of Public Health, has designed Health Policy and universal health insurance programs for China, Colombia, Cyprus, Hong Kong, Malaysia, Poland, South Africa, Sweden, Taiwan, Uganda and Vietnam. He also developed a single-payer universal insurance model for Vermont.
Americans have long resisted single payer because we value individual liberty and choice, Hsiao said. “But we blindly apply this ideal to everything,” he added. In health care, we rely on market competition and patient choice, but the result is administrative costs that are four to five times higher than those of other rich nations, he explained.
By his estimates, single payer would save more than $800 billion in health care spending annually, including $500 billion in administrative costs, $150 billion in fraud and abuse payments and $150 billion in costs for pharmaceuticals. “How do I know this,” he asked. “Because I have done this work in other countries.”
While the savings are attractive, a single-payer health care system would require increased revenue, likely in the form of higher taxes on wages and on corporations’ gross income, he said, adding that is important to note that a single-payer system would enable Americans to pay much less for health insurance premiums and out-of-pocket payments. Employers also would pay less for health care for their workers, producing more in savings than Americans would pay in higher taxes.
Even though Americans would experience net savings from single payer, the need to explain this somewhat complicated math is likely to cause politicians to avoid the subject, he concluded.
Background
- Bernie, single payer – and a little Hillary fact checking.
- News coverage should reflect that Vermont has long road ahead to single-payer system.
Upcoming Webcast: Peter Shumlin, former governor of Vermont, “In Pursuit of a Single-Payer Plan: Lessons Learned,” Tuesday, Sept. 19, 12 to 12:30 pm EST.



