
Physicians treating pregnant women/people needing emergency medical care are wrestling with how to comply with what’s been called the bedrock law of emergency medicine when facing strict, new mandates on abortion.
“Confusion among emergency room doctors remains even after the Biden administration clarified this week that federal law allowing abortions in life-or-death situations supersedes any restrictions a state may have on the procedure,” Tony Pugh wrote for Bloomberg Law on Wednesday. His article explained how conflicting federal and state laws are complicating abortion care.
Early this week, Melanie Evans of The Wall Street Journal took a close look at how physicians and hospitals are addressing the mandates of the Emergency Medical Treatment and Active Labor Act (EMTALA) of 1986 in the wake of the overturning of Roe v. Wade. That decision in Dobbs v. Jackson Women’s Health Organization stripped away an almost 50-year-old right to an abortion.
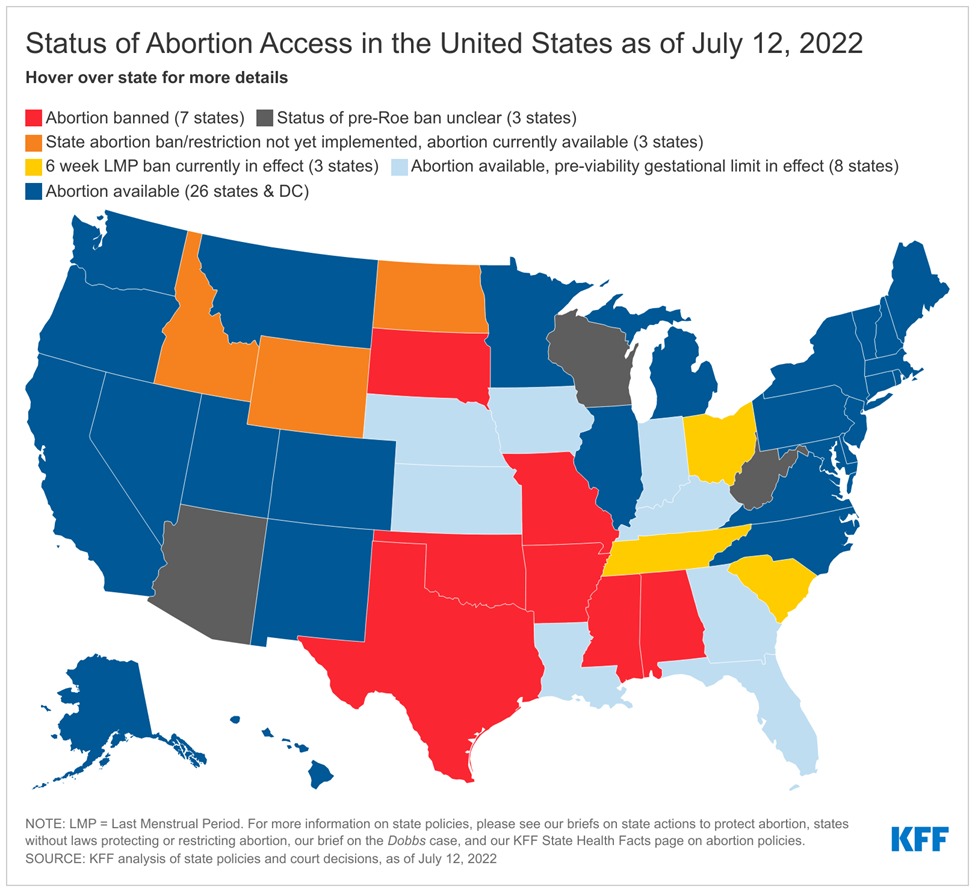
Even before the SCOTUS decision on June 24, many states had enacted laws to either restrict or prohibit abortions or expand and protect access to abortion in anticipation of the ruling to overturn Roe v. Wade, as noted in the nonprofit Kaiser Family Foundation’s tracker of these measures.
Although EMTALA preempts state law, relying on that law alone does not eliminate the confusion or legal exposure that physicians face, Evans reported. Doctors and lawyers told Evans that the mismatch between federal law and state bans or restrictions on abortions leaves hospitals to decide whether to follow one law over another depending on how much legal risk they’re willing to accept.
“Physicians, meantime, could be left to make difficult decisions about whether to delay emergency treatment until a woman’s condition worsens enough to satisfy state or federal law requirements for performing an abortion, the doctors and lawyers said,” Evans wrote.
One Wednesday (July 13, Scott Wilson reported for The Washington Post that prosecutors in some cities in Republican-controlled states said they will not enforce bans on abortion in states that impose them. Also on Wednesday, Myah Ward reported for Politico that Todd Rotika, Indiana’s attorney general, said his office planned to investigate the Indiana doctor who helped a 10-year-old rape victim who crossed state lines to have an abortion.
Seeking to provide some clarity, the Biden administration announced on Monday (July 11) that the federal government would use its clout as a major purchaser of health care to address the issue. That day, Health and Human Services Secretary Xavier Becerra and the federal Centers for Medicare and Medicaid Services (CMS) issued statements explaining how denying emergency care to pregnant/women people, including those needing an abortion, could result in a loss of Medicare, Medicaid and other funding.
The next day (July 12), the U.S. Department of Justice announced the formation of the Reproductive Rights Task Force to make formal that department’s work to protect reproductive freedom under federal law.
In his July 11 letter to clinicians, Becerra wrote that, in general, EMTALA requires hospitals to provide people in emergencies with appropriate medical screening examinations, stabilizing treatment and transfer. Emergency medical conditions involving pregnant patients may include ectopic pregnancy and complications of a miscarriage.
Treatment needed to stabilize people in these cases could include abortion, removal of one or both fallopian tubes and methotrexate therapy, wrote Becerra, an attorney who is married to an obstetrician.
Enforcement of EMTALA begins with a complaint. “If the results of a complaint investigation indicate that a hospital violated one or more of the provisions of EMTALA, a hospital may be subject to termination of its Medicare provider agreement and/or the imposition of civil monetary penalties,” Becerra wrote. If doctors or hospitals violate EMTALA, they could be excluded from Medicare and state health care programs, he added.
That same day, CMS sent a memo reminding hospitals of their obligations to patients under EMTALA, making similar arguments. “Under this same authority, HHS … may also exclude physicians from participation in Medicare and state health care programs. CMS may also penalize a hospital by terminating its provider agreement.”
A CMS spokesperson explained that state health care programs include Medicaid, CHIP and other similar initiatives, such as Basic Health Programs.
In a recent blog post, Jeffrey Davis, the director of regulatory affairs for the American College of Emergency Physicians, explained the challenges doctors may face when seeking to reconcile EMTALA against state abortion laws. In the United States, EMTALA is the “bedrock law and the foundation of the emergency care safety net,” he wrote. Even under the new guidance from CMS, gray areas remain in emergencies when state laws prohibit abortion, he added.
“A Preview of the Dangerous Future of Abortion Bans”
For the WSJ, Evans noted research that the New England Journal of Medicine published in perspective article on June 22, “A Preview of the Dangerous Future of Abortion Bans — Texas Senate Bill 8.”
After the Texas legislature implemented a near-total ban on abortion last year, physicians in the Lone Star State told researchers that their fear of penalties under the law led them to delay medical care in multiple cases until a pregnant woman’s symptoms worsened.
To date, the Texas experience shows how patients with complex pregnancies may confront diverse interpretations of state laws that will result in unequal access to care, the researchers wrote.
The health risks for pregnant women/people rise sharply while physicians wait for symptoms to worsen, and delays could lead to death from blood loss or infection, Evans noted.
Dana Stone, M.D., an obstetrician-gynecologist in Oklahoma City, told Evans, “It’s not theoretical for us. We know how terrifying it can be when things get out of hand.”
Lacking clear legal guidance, Stone cannot be confident which procedures would be legal, she said. “In practice, we will have to pick up the phone and call the attorney before we take care of a woman,” she told Evans.
Physicians treating pregnant women/people in Florida also may face legal jeopardy, according to reporting from Verónica Zaragovia for radio station WLRN in Miami.
As in Texas, doctors in South Florida say a new state law banning most abortions after 15 weeks could harm patients and providers in part because the law leaves health care providers with fewer options than they had before the legislature passed the new law.
While the law bans most abortions after 15 weeks, there are some exceptions, Zaragovia wrote. One exception would be if two physicians agree that a fetus or the patient could die, she reported. “The legislation doesn’t explain how imminent that danger needs to be,” she added.
Additional information to aid reporting
- On July 8, President Biden signed a broad plan, known as an executive order, to preserve access to abortion, mandating that HHS report within 30 days how to expand access to medication abortion and emergency contraception; required the departments of Justice and Homeland Security to ensure the safety of medical clinics delivering reproductive and related health care services; requested that HHS, DOJ and the Federal Trade Commission seek ways to prevent digital surveillance related to reproductive health care services; Asked the DOJ to encourage private pro bono attorneys, bar associations and public interest groups to represent and assist patients, clinicians and organizations involved in reproductive health services.
- In May, five journalists for The Guardian recapped five cases in countries outside of the United States where women died after not getting the care they needed during obstetric crises. Among these cases was one that triggered Ireland’s 2018 repeal its near-total ban on abortion.



