The Affordable Care Act created many opportunities for Medicare to test new ways of paying for health care. One of the biggest and most dramatic tests is now getting underway: bundled payments for hip or knee replacement.
Unlike most Center for Medicaid and Medicare Innovation (CMMI) projects on payment and delivery reform, this one is mandatory for hospitals in 67 geographic areas designated as participants. The test began April 1 and is supposed to run for five years.
The model holds the participating hospitals financially accountable for the entire “episode” of care – from admission through 90 days of rehab and recovery. It will require cooperation and collaboration among doctors, hospitals, home health, physical therapy and nursing homes. It covers all the services under Medicare Part A and B per episode (there are a few exceptions). It won’t be the same amount for every patient across the country, depending on regional costs and whether the surgery is an elective joint replacement or an emergency hip fracture.
Hospitals could get extra money if they do well on total costs – and may have to repay Medicare if they overspend (although not during the first year). Melinda Beck from The Wall Street Journal wrote a very good overview of how doctors, hospitals and nursing homes are affected, particularly interesting since there are some fee-for-service payments within the bundling project.
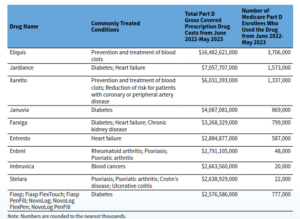
In 2014, more than 400,000 of these procedures took place, costing more than $7 billion for the hospitalizations alone, and not including rehabilitation and recovery. Costs vary tremendously – within and among geographic areas – as do rate of infections or complications such as implant failures after surgery. The use of skilled nursing facilities (SNF) for recovery compared with care at home also varies tremendously, as does the cost. Medicare costs ranges from $16,500 to $33,000 across geographic areas.
This new process is designed to both save money and improve care coordination, particularly through the transition from hospital to home or nursing facility. Here are some questions to ask as you explore how the health care community in your area is – or isn’t – taking part:
- How much resistance has there been and from whom?
- How is it affecting hospitals, physicians and skilled nursing facilities?
- What kinds of changes to care, and care coordination, are underway?
- What resources are hospitals drawing on to make the changes? Are they re-inventing the wheel rather from learning from good models?
- Is there any indication – as some orthopedists have warned – that sicker patients are being waved away from elective joint replacement because they are potentially costlier and complex?
- Are there educational sessions for pre-surgery patients to promote better recovery (a practice some leading hospitals have been doing for some time)?
- Is there a trip to a patient’s homes before surgery to assess what the person would need to recover safely there, rather than in a nursing facility?
- If your community is not taking part in the test, are they adopting some of these practices voluntarily to improve outcomes and share costs?
Resources:
- A summary from CMMI.
- An overview of CMS bundling initiatives – not just this one – in a Health Affairs/RWJF issue brief.
- A very good overview by Melanie Evans in Modern Healthcare.
- This story from the Naples Daily News in Florida provides a good taste of physician skepticism and resistance. (They will have to collaborate with post-acute care providers in ways that most are not accustomed to.) It would have been interesting to read more about what changes the hospitals are considering other than starting task forces and studying the problem.
- Tip sheet: How to gauge ‘success’ at CMMI
- Tip sheet: Latest innovations in Medicare