

If you saw our November webcast on how consumers and payers can evaluate physician quality, you know that we began with a quote from Atul Gawande, M.D., about patient outcomes.
A professor of health policy and management at Harvard University and a prolific and gifted writer, Gawande is the best-selling author of “Being Mortal” and “The Checklist Manifesto.” He’s also a contributor for The New Yorker and other publications, writing about cardiologists in McAllen, Texas, super utilizers in New Jersey, and unnecessary care nationwide.
In short, he’s darn good at what we do.
No, we don’t know how to do it. In most states, it’s all but impossible to evaluate outcomes based on physician quality, as Francois de Brantes, executive director of the Health Care Incentives Improvement Institute explained in our webcast. Last week, HCI3 released its third State Report Card on Transparency of Physician Quality Information. In the report card, HCI3 gave failing grades to 43 states for providing inadequate information to consumers on the quality of physician care. Three states (California, Minnesota and Washington state) got an A, Maine got a B, and three states (Massachusetts, Oregon and Wisconsin) got a C. Among all other states, three (Missouri, New Mexico and Ohio) got a D; the remaining 40 got an F.
Even in the best-scoring states, consumers get quality information on fewer than half of all physicians because there’s little data on meaningful measures for specialty care. Even for the specialties that have quality measures, many are not meaningful to consumers. “The upshot is that the decks have been stacked on the side of providers, not consumers. But that’s about to change,” the report says.
In a white paper that accompanied the report card, HCI3 described the methodology it developed and has refined for 10 years, saying:
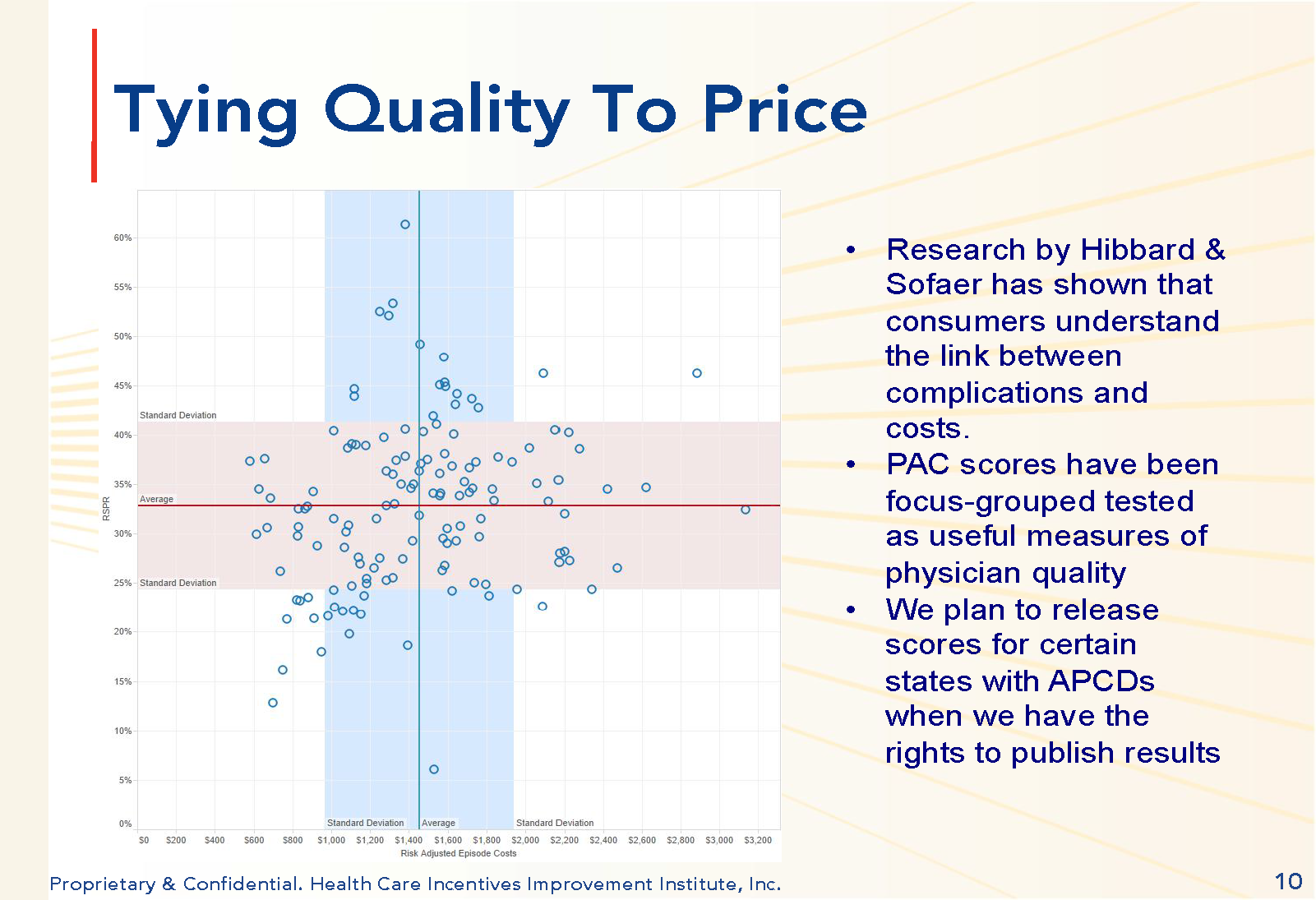
“Our work has focused on defining potentially avoidable complications (PACs) for a large number of routine chronic conditions, procedures and acute medical events. It’s from those definitions that we can calculate rates of avoidable complications and then adjust them for the severity of the patient’s condition and general health. What you end up with is a reliable way of differentiating provider performance.
“What this means is that any state with an all-payer claims database, any public or private health plan, and any employer with enough employees, can now calculate and publish comparative quality of physicians. And if they were to tie this measure to costs of care, you would end up with a real value score, one that consumers can understand.” (See Figure: Tying Physician Quality to Price.)
Using HCI3’s methodology, consumers, payers and others can measure risk-adjusted rates of complications for any number of medical conditions, illnesses, procedures and other medical episodes of care, the report card says.
For information on HCI3’s methodology, watch the recording of the AHCJ webcast and download the white paper, “Piercing the Darkness: A Generalizable Approach To Reliably Measuring Quality Of Care.”








