

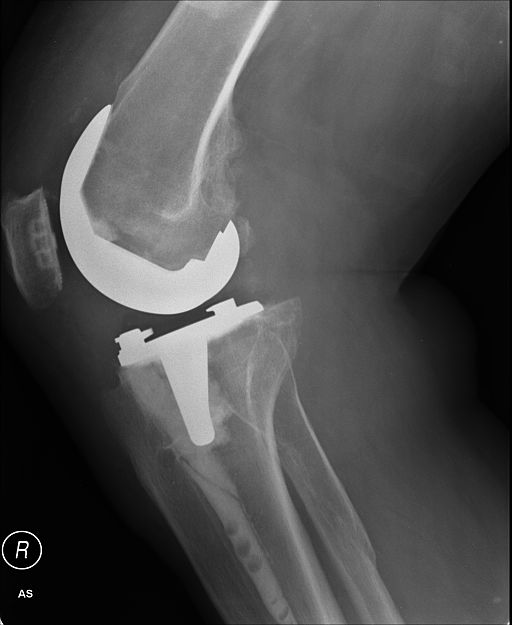
Earlier this month, the federal Centers for Medicare & Medicaid Services proposed a five-year bundled-payment test program for hip and knee replacement surgeries.
At the time, CMS said its Comprehensive Care for Joint Replacement (CCJR) program would require 800 hospitals in 75 areas to test bundled payments for most of the 100,000 hip and knee surgeries that Medicare covers annually.
The proposal, which we covered here, would allow CMS to eliminate some of the widespread variation in costs and offer one more way for the Obama administration to squeeze out fee-for-service reimbursement by transforming payment from volume to value, CMS said. Currently the agency is soliciting comments on its proposal (PDF) until Sept. 8, and expects to implementt he program Jan. 1.
Among the comments CMS will get will be a blistering critique from Harold Miller, the president and CEO of the Center for Healthcare Quality and Payment Reform, In a policy brief, “Bundling Badly: Problems with Medicare’s Comprehensive Care for Joint Replacement Proposal,” Miller explained that the plan may not be as well designed as CMS would have us believe.
Among seven specific criticisms are two that are potentially detrimental to the health care system itself. First, the proposal would encourage further consolidation in health care, fewer choices for consumers, and higher prices, he wrote. Second, it would encourage unnecessary hip and knee surgeries while discouraging physicians and hospitals from developing innovative approaches to managing patients’ hip and knee pain, he added.
The four-page report is well worth reading because it explains bundled payment thoroughly and clearly and because it takes apart the CCJR proposal in detail. Here are Miller’s seven criticisms:
- True episode payment would be desirable, but this is just P4P (pay for performance)
- It may look like bundled payment but it isn’t really
- It’s a payment design that penalizes innovation instead of encouraging it
- CCJR will likely accelerate provider consolidation and increase prices for private payers
- Poorly designed risk adjustment could reduce access and result in more unnecessary surgeries
- There’s no reward for higher quality; just smaller bonuses if quality is low
- A mandatory “test” would preclude other, better approaches.
To assess whether Miller’s criticisms are on target or not, I asked Francois de Brantes, the executive director of the Health Care Incentives Improvement Institute, for his opinion. Few health policy experts know more about bundled payment than de Brantes given that HCI3 has been implementing its form of bundled payments (called the Prometheus Payment model) since 2007.
“He’s mostly right,” de Brantes said. “The one area I disagree with is that it will accelerate provider consolidation. There’s no real evidence of that in bundled payment programs, but the other points he brings up are correct. So while CCJR is a strong signal to providers that fee-for-service is ending, the design of the program is flawed.
“We’ve spent the past several years alerting CMS to the flaws in its Bundled Payment for Care Initiative program (on which CCJR is based), and they’ve ignored all of the comments and suggestions,” he added.





{kind=link}