


The Affordable Care Act requires all state Medicaid programs – whether they opted into expansion or not – to help people quit smoking. The law requires at least some counseling and FDA-approved therapies, including nicotine gum and some drugs that assist in tobacco cessation.
How are the states doing? Not great.
Researchers from the Milken Institute School of Public Health at George Washington University estimate that only one in 10 smokers on Medicaid are getting anti-smoking medication. Many states put up obstacles that make it harder for people to get the drugs that might block their cravings and help them quit, according to research discussed in the January edition of Health Affairs (Note: Link is to abstract. Free full access available for AHCJ members – see registration information here.)
“These data show that most Medicaid programs could do much more to help smokers quit,” Leighton Ku, Ph.D., M.P.H., interim chair of the department of health policy and management at the public health school and the study’s lead author, said in a release about the study. “Data from the Centers for Disease Control and Prevention suggests that medical treatments for smoking-related diseases will cost the Medicaid program about $75 billion in 2016, but we spend less than one-quarter of one percent of that amount to help smokers quit.”
An estimated one-third of adult Medicaid beneficiaries smoke – about twice as many as the overall adult population.
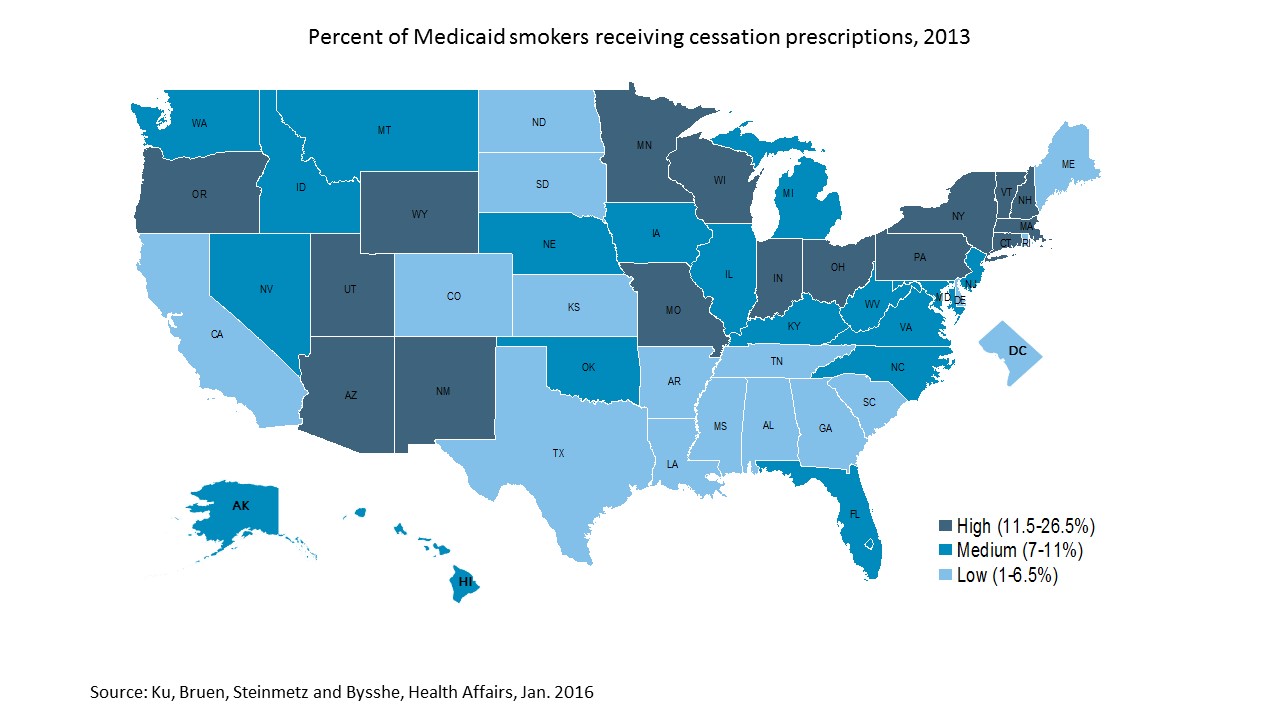
The study found that states vary a great deal in how much states enable easy access to drugs that might help these people quit. Nearly one in three Medicaid smokers in Minnesota get them, versus less than one percent in Texas. States may also create cumbersome barriers – cost-sharing, or the need to get prior authorization.
States that use – or don’t use – the cessation treatments don’t necessarily fall on blue-red state lines. The study found the top five states in 2013 were Minnesota, New Hampshire, Utah, Oregon and Arizona. The bottom five were Texas, Rhode Island, Kansas, Mississippi and Arkansas. In both those categories, some of the states have expanded Medicaid but others have not.
Researchers say that spending the money on cessation can pay off quickly for instance by reducing hospitalization for heart disease.
“Tobacco is addictive,” Ku and his colleagues said in the Health Affairs article. “Stopping smoking is difficult, and attempts to quit are often short-lived. Nonetheless, efforts to quit are an effective way to reduce the health consequences and medical costs of smoking, and even temporary breaks from smoking can be helpful. … Increasing tobacco cessation efforts among Medicaid enrollees is a key public health objective.”
The study did find some differences between states that have expanded Medicaid and those that have not – although the differences have roots that stretch back a number of years so aren’t all because of the ACA. But states that do expand do have broader opportunities to help smokers quit:
“Medicaid expansion states usually have lower smoking prevalence and greater use of tobacco cessation, compared to non-expansion states,” the team wrote. “We do not believe that differences in smoking or tobacco cessation rates are caused by states’ decisions about expanding Medicaid. These patterns began long before those decisions were made, and there are examples of high and low smoking prevalence and cessation among both expanding and nonexpanding states.
Nonetheless, the differences have serious public health consequences. By covering more people, expansion states make tobacco cessation more broadly available, expanding its potential public health impact. Non-expansion states cover fewer people and already have higher smoking prevalence, so they will experience a greater health burden, compared to expansion states.”
This is an easy story to localize for your state:
- How does it rate in comparison to other states?
- What obstacles exist to obtaining help quitting – and is anyone talking about reducing them?
- Do clinics and doctors know that Medicaid covers these services?
- Is anyone spreading the word among smokers themselves?
- How about the Quit Help lines. Do they proactively say what kind of help callers can get? Or are both patients and providers too fatalistic, believing it’s just too hard?




