At a conference last year, Michael Laposata, M.D., Ph.D., one of the nation’s best known pathologists, explained how clinical laboratories could deliver more value to patients, physicians, and health insurers. To do so, pathologists and laboratory scientists need to provide more detailed explanations about lab test results because even physicians who order genetic and molecular tests are often confused about the results, said Laposata, chairman of the Department of Pathology at the University of Texas Medical Branch.
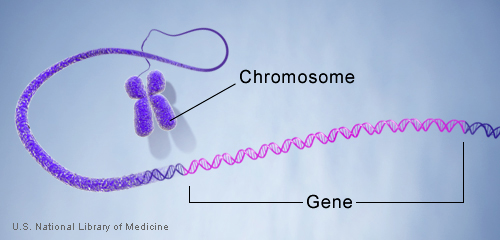
When he explains test results to ordering physicians, he frequently refers to an “allele” which is one of two or more versions of a gene, he said. When he does, physicians sometimes ask, “What’s an allele?”
His anecdote is telling following President Obama’s announcement last month that he recommended spending $215 million on the precision medicine initiative. The announcement was correctly hailed as an important and needed investment in medical technology. “Precision medicine” is described by the National Institutes of Health as “an emerging approach for disease treatment and prevention that takes into account individual variability in genes, environment, and lifestyle for each person.”
Given that there is and will continue to be a lot of hype about precision and personalized medicine, we may want to check our expectations, because the hurdles are daunting, as Tabitha M. Powledge wrote for the Genetic Literacy Project. “The plan embodies a wonderfully human let’s-climb-Everest-because-it’s-there aspiration. But you also have to wonder about the practicality of such a sweeping program,” she explained.
Writing for Genomeweb, journalist Turna Ray outlined some of the hurdles clinicians will face, saying personalized medicine already has a credibility problem. For example, researchers behind the Human Genome Project overpromised what could be gained from their international research effort to determine the DNA sequence of the entire human genome, she wrote.
In her thorough examination of the hope and promise of Obama’s precision medicine initiative, Ray quoted Hank Greely, a law professor at Stanford University, who has studied biomedical advances. “There is not much good, proven, scientific, medical uses for what we’re talking about as personalized or precision medicine,” Greely said. “And yet, we … sell and we hype as if there is much more.”
Ray also reported that Obama’s proposal follows the National Institutes of Health’s decision last year to kill the National Children’s Study. “The study, which the government launched in 2005 to much drumbeating, was canceled in December after spending $1 billion,” she wrote. In this initiative, researchers analyzed the long-term environmental and biological factors that affect the health of 100,000 children.
In December, John Tozzi and Alex Wayne wrote for Bloomberg Business, “How the U.S. Government Botched Its Multibillion-Dollar Plan to Beat Childhood Disease.” As Tozzi and Wayne did, journalists covering genomic medicine and the president’s initiative will need to separate facts from hype.
Michael Millenson made this point when he wrote about Obama’s proposal for Forbes, explaining that covering genomic medicine is harder than it looks. In a follow-up email to me, he said: “Here’s the problem: because personalized medicine is in the realm of OMG-that’s-too-complicated science, the usual watchdogs don’t see it. Plus the big academic medical centers love the grants that it generates.”
Even health insurers are struggling to understand the full implications of genetic and molecular testing, and so it’s incumbent on journalists to look critically at all developments in this field, Millenson added.
For an example of excellent reporting in this field, read what Beth Daley and Shan Wang wrote in December for the New England Center for Investigative Reporting. Their work explained how genetic screening tests may be oversold and are often misunderstood and how a recent experiment raised questions about genetic screening labs. They also showed how patients and physicians were not fully aware of what genetic screening tests can and cannot do. We covered their reporting here.